

when a familiar voice cut through the din of the subway car.
“Alyssa?” Her father’s voice was unmistakable, even above the clatter of the train. She looked up, startled, to see him standing a few feet away, concern etched across his face.
“Dad? What are you doing here?” Her voice cracked with a mix of surprise and relief, even as her son continued to wail on her shoulder.
“I could ask you the same thing,” he replied, glancing at the stroller and the two children bundled in layers to keep out the cold. “Why aren’t you using the car I gave you?”
Alyssa took a deep breath, trying to find the right words to explain the complex web of family dynamics that had left her without the one thing her father had given her for her safety and convenience. She recounted the saga of the car, the endless excuses, and finally, the hostile words from Jordan.
Her father listened in silence, his expression growing more serious as she continued. When she finished, he simply said, “Don’t worry, Alyssa.”
Those two words, so simple and yet so powerful, were a balm to her frayed nerves. Her father had always been a man of few words, but when he spoke, his words carried weight. She felt a flicker of hope ignite within her—a hope that perhaps things could change.
That evening, her father arrived at her apartment, a determined look in his eyes. He asked Alyssa to stay home with the kids while he went to have a conversation with Jordan. A part of her was anxious about the encounter—she didn’t want to cause trouble or escalate the tension. But another part, a stronger part, felt a surge of relief and empowerment. She had someone on her side.
The confrontation between her father and Jordan was not as dramatic as Alyssa had feared. Her father was calm but firm, reminding Jordan of the reason he had given Alyssa the car in the first place—to provide a secure and efficient way for his daughter and grandchildren to navigate their lives. He emphasized the importance of respecting Alyssa’s needs and decisions, especially when it came to family resources.
Jordan, perhaps taken aback by the unexpected intervention, promised to return the car the following day. True to his word, the keys were back in Alyssa’s hands the next morning. It was a small victory, but it felt monumental.
With the SUV back, Alyssa’s routine transformed. No longer did she have to struggle with the bus or subway; no longer did she have to endure the biting cold with two small children. The freedom of mobility brought a newfound sense of independence and confidence.
Over the following weeks, Alyssa reflected on her father’s simple act of standing up for her. It was a reminder of the strength of family bonds—real family bonds, built on respect and support rather than obligation and control. She realized that while she might have married into the Reynolds family, she still had her family’s love and support to rely on.
In the end, the experience taught Alyssa about the power of standing up for herself and the importance of setting boundaries, even with those she cared about. Her father’s intervention was the catalyst she needed to reclaim her voice, and she vowed to never let it be silenced again.


I sat down with a heaviness in my chest, the weight of the unknown pressing on me. The room seemed to close in as I braced myself for whatever revelation lay in that file. The doctor’s voice was calm, but his eyes were serious. “The baby you found is your grandson, Mrs. Reynolds. Genetically, he is the son of Lewis.”
The words hit me like a cold wave. I had been mourning a son, and now I was told that part of him lived on in this tiny, fragile life. My mind raced, trying to piece together how such a secret could have been kept. Cynthia had never spoken of a pregnancy, never hinted at the possibility. How could she have hidden something so monumental, so life-altering?
The detective took over, explaining that they were investigating why Cynthia had chosen such a drastic action. There was talk of postpartum issues, of stress from the loss of Lewis that had driven her to desperation. But none of it made sense to me. The Cynthia I had known was strong and capable—at least, that was the facade she had shown.
Over the next few days, I found myself wrestling with anger and confusion. How had I not seen the signs? Why hadn’t she come to me for help? As I spent more time at the hospital, sitting beside the incubator where my grandson lay, I tried to focus on the fragile thread of hope. He was small, but the doctors assured me he was a fighter.
Cynthia was found a few days later, staying with a friend in a nearby town. She was in a state of emotional turmoil, the weight of her actions pressing down on her. The authorities had intervened, and she faced a psychiatric evaluation, a necessary step before determining the future for her and the child.
As I navigated the new reality, I spent long hours thinking about family, about the secrets we keep, and how they can shape our lives. I thought about Lewis and the joy he would have felt knowing he had a son, a continuation of his legacy despite the tragedy that had taken him from us.
Family meetings with social workers and legal advisors filled the days. I found myself at the center of this unfolding drama, a twist of fate that had returned a piece of my son to me. It was decided that I would take temporary custody of the baby, giving Cynthia the space and time to heal.
The first night I brought him home, I sat in Lewis’s old room, rocking my grandson to sleep. His tiny fingers curled around mine, and I felt a surge of determination. This child, a testament to my son’s existence, deserved a chance at a life filled with love and security.
In the months that followed, our family began to heal. Cynthia, with the help of therapy, slowly pieced herself back together. She visited often, and we started to rebuild a relationship founded on understanding and forgiveness. The past could not be changed, but we could learn from it, grow beyond it.
As I watched my grandson grow, his laughter echoing through the house that had once been so silent, I realized that life has a way of surprising us, of bringing light even in the darkest of times. The secrets that had once threatened to tear us apart had instead revealed the strength of our bonds, and for that, I was grateful.
As speculation swirled about his supposed frailty, Tom Selleck refused to let rumors write his final chapter. Behind the calm authority of Commissioner Frank Reagan is a 76-year-old man managing relentless arthritis, relying on carefully monitored steroids just to keep moving. Every scene, every step on Blue Bloods now comes with calculation and cost, but also with a stubborn, almost defiant gratitude.
Rather than retreat from the spotlight, he chose transparency over mystery. He acknowledged the pain, admitted the struggle, yet made one thing crystal clear: he is not done. His promise that Blue Bloods will continue with him is more than a career decision; it’s a declaration of purpose. To fans who feared a quiet disappearance, Selleck offers something rarer—a man aging in public, refusing to surrender the work and character he loves.
Rather than retreat from the spotlight, he chose transparency over mystery. He acknowledged the pain, admitted the struggle, yet made one thing crystal clear: he is not done. His promise that Blue Bloods will continue with him is more than a career decision; it’s a declaration of purpose. To fans who feared a quiet disappearance, Selleck offers something rarer—a man aging in public, refusing to surrender the work and character he loves.
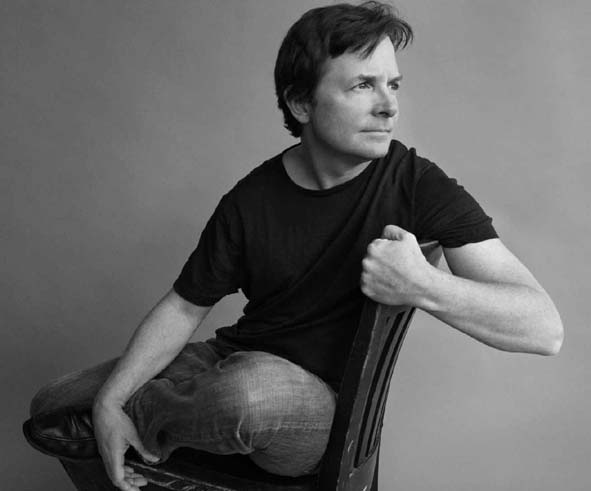
Michael J. Fox is one of the most recognizable faces in popular culture — an actor whose likable screen presence, quick wit, and undeniable charm made him a household name in the 1980s and beyond.
At a time when movies and television were shaping the dreams of millions, Fox’s performances struck a chord, captivating audiences around the world and establishing him as one of Hollywood’s most beloved talents.
Yet his life story is far more than a chronicle of early success. It’s also a story of resilience, advocacy, hope, and transformation in the face of a life‑altering challenge. Michael Andrew Fox was born on June 9, 1961, in Edmonton, Alberta, Canada.
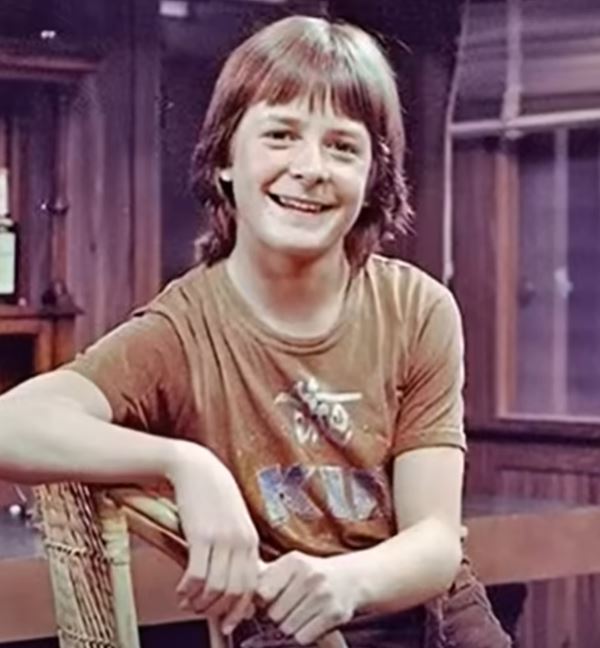
He grew up with a love of performance and a sense of humor that would later define much of his screen work. As a teenager, he appeared in local television and theatre, building experience that carried him to the United States to pursue a professional acting career.
After moving to Los Angeles as a young man, he faced the typical struggles of an aspiring actor. In Hollywood, he learned quickly that success rarely comes easily.
Nonetheless, his persistence paid off when he landed the role of Alex P. Keaton on the popular NBC sitcom Family Ties, which debuted in 1982.
On Family Ties, Fox played the intelligent, fast‑talking, conservative‑leaning teenage son of liberal parents. His performance was both comedic and charismatic, earning him widespread praise and several awards, including multiple Emmy Awards and Golden Globes during the show’s run. The role also made him a star — not just in America, but internationally.
Breakthrough: Back to the Future and Film Success
While Fox’s television success with Family Ties firmly established him in the entertainment world, it was the 1985 blockbuster Back to the Future that turned him into a global movie star.
In the film, he portrayed Marty McFly, a teenager accidentally sent back in time in a DeLorean time machine. The role became iconic, capturing the imagination of audiences and launching a major franchise.
Fox’s work in Back to the Future required high energy, physicality, and a natural comedic timing — all of which he delivered with ease. He juggled filming for the movie with his television commitments, a feat that spoke to both his passion and work ethic.
Over the next several years, he starred in a string of successful films, including Teen Wolf, The Secret of My Success, Casualties of War, and the Back to the Future sequels.
By the age of 29, Fox had spent most of his adult life in front of the camera, winning over viewers with his mix of humor, vulnerability, and relatable charm.
A Devastating Diagnosis
In 1991, during filming on the set of Doc Hollywood, Fox began noticing a tremor in his pinky finger. What seemed at first like a minor concern was diagnosed by a neurologist as early‑onset Parkinson’s disease, a progressive neurological condition that affects movement and coordination.
He was just 29 years old — an age when most people are still building careers and planning for the future.
Parkinson’s disease is a degenerative disorder without a cure, and its symptoms — including tremors, stiffness, and difficulty with balance and speech — can worsen over time.
For someone whose life and career depended on precise movement, engaging performance, and public presence, this diagnosis was nothing short of life‑altering.
Initially, Fox kept the diagnosis private. He continued acting, including starring as Deputy Mayor Mike Flaherty on the ABC sitcom Spin City beginning in 1996, where he received further critical acclaim and awards.
Behind the scenes, however, he struggled with the reality of the disease, entering what he later would describe as several years of denial and internal conflict about his future.
Going Public and Becoming an Advocate
For years, Fox tried to manage his symptoms and maintain his career without revealing the truth about his health. Eventually, however, he realized that keeping the diagnosis secret was no longer tenable.
In 1998, during his run on Spin City, he publicly disclosed that he had Parkinson’s disease in an interview with People magazine and ABC’s Barbara Walters. This courageous decision helped break down stigma and opened up a national conversation about the disease.

The response he received — both from fans and from the broader entertainment community — was deeply supportive, emboldening Fox to shift his focus from hiding his symptoms to advocating for research and understanding. Rather than retreating from the world, he chose to use his platform to make a difference.
Two years after publicly revealing his diagnosis, in 2000, Fox founded The Michael J. Fox Foundation for Parkinson’s Research.
Today, the organization is one of the world’s leading non‑profit funders of Parkinson’s research, having raised billions of dollars and supported groundbreaking clinical studies, early‑stage therapeutic development, and the largest datasets of biosamples ever assembled for Parkinson’s research.
Fox’s foundation has also contributed to research that aims to detect the disease earlier and understand its progression more deeply — milestones that could one day lead to more effective treatments or prevention.
While a cure has not yet been found, the progress made in research has been substantial and remains a testament to sustained advocacy and investment.
Beyond Parkinson’s: Continued Career and Personal Life
Even as his symptoms gradually became more noticeable, Fox continued working in film and television. In addition to Spin City, he voiced lead characters in animated films such as Stuart Little and appeared in roles on series like Rescue Me, The Good Wife, Curb Your Enthusiasm, and The Good Fight.
His final major television project as a regular cast member was The Michael J. Fox Show from 2013 to 2014.

Over time, however, Parkinson’s symptoms made the physical demands of acting increasingly difficult. In 2020, he announced his retirement from full‑time acting due to the progression of his condition.
Though retired, Fox made a notable return to the screen, portraying a character with Parkinson’s disease in the Apple TV+ series Shrinking, demonstrating both empathy and courage in bringing an honest portrayal to audiences.
Fox’s personal life has been a grounding force through his journey. He married actress Tracy Pollan, his co‑star from Family Ties, in 1988, and they have four children together.
Fox has frequently spoken about the critical role his family has played in supporting him through the highs and lows of his health challenges and advocacy work.
Writing and Reflecting: Memoirs and Legacy
Michael J. Fox has authored several books that offer insight into his life, career, and evolving relationship with Parkinson’s disease. His first memoir, Lucky Man, chronicles his rise to fame and early years living with Parkinson’s.
The book combines candid reflections on vulnerability with his characteristic humor and philosophical insight, presenting both the high points of his success and the challenges of confronting a chronic illness.
He later published other works, including Always Looking Up and No Time Like the Future: An Optimist Considers Mortality, which explore deeper themes of resilience, mortality, and the meaning of purpose amidst adversity. These writings have resonated with readers worldwide, offering both perspective and inspiration.
In 2025, he announced a new memoir titled Future Boy, aiming to look back at his early career and the experiences that shaped him, including the joys and challenges of simultaneously filming Family Ties and Back to the Future.

Recognition and Honors
Over the course of his career and advocacy, Fox has been recognized with numerous awards. As an actor, he won multiple Emmys, Golden Globes, Screen Actors Guild Awards, and even a Grammy for contributions to entertainment.
He was inducted into the Hollywood Walk of Fame and Canada’s Walk of Fame, and he was appointed an Officer of the Order of Canada for his contributions to film and television as well as his humanitarian work.
Perhaps most notably, in 2022, Fox received the Jean Hersholt Humanitarian Award from the Academy of Motion Picture Arts and Sciences — an honorary Oscar recognizing his advocacy and philanthropic contributions in the fight against Parkinson’s disease.
The Ongoing Journey: Challenges and Perspective
Living with Parkinson’s for more than three decades has not been easy. The disease is degenerative, affecting movement, balance, coordination, and even speech.
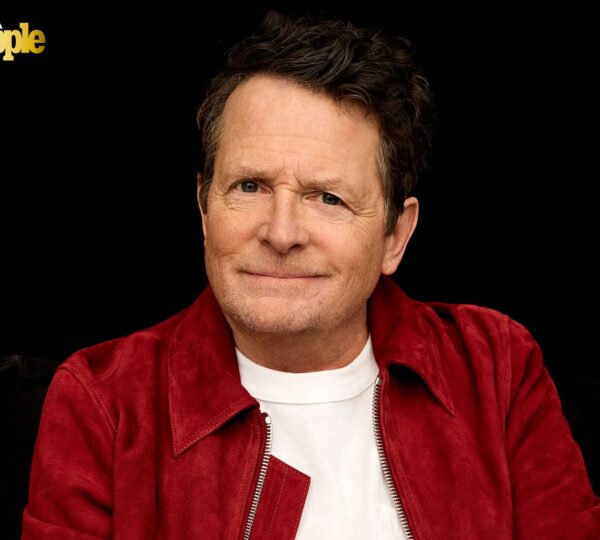
Fox has spoken openly about the daily challenges it presents — including the emotional and physical toll — yet he approaches it with unflinching honesty and a sense of optimism that has defined his public persona.
In recent interviews, Fox has discussed how he navigates daily life with Parkinson’s, including using a wheelchair and managing his symptoms with medication and therapy.
Despite these hurdles, he continues to find meaning in family, advocacy, and creative expression. His partnership with his wife, Tracy Pollan, and their children remains a central source of strength.
A Legacy of Hope and Inspiration
Michael J. Fox’s life story is a powerful reminder that talent and success are only part of a person’s narrative. His trajectory from teenage TV star to Hollywood legend and then to a tireless advocate for Parkinson’s research reflects not only his gifts as a performer but his deep humanity, resilience, and capacity for hope.
He has shown the world that adversity — even one as challenging as a chronic, progressive disease — can be met with courage, purpose, and an unshakeable commitment to making life better for others.
In doing so, Fox has inspired millions of people living with Parkinson’s and beyond, proving that while a diagnosis might change a life, it does not have to define it.
At a time when movies and television were shaping the dreams of millions, Fox’s performances struck a chord, captivating audiences around the world and establishing him as one of Hollywood’s most beloved talents.
Yet his life story is far more than a chronicle of early success. It’s also a story of resilience, advocacy, hope, and transformation in the face of a life‑altering challenge. Michael Andrew Fox was born on June 9, 1961, in Edmonton, Alberta, Canada.
He grew up with a love of performance and a sense of humor that would later define much of his screen work. As a teenager, he appeared in local television and theatre, building experience that carried him to the United States to pursue a professional acting career.
After moving to Los Angeles as a young man, he faced the typical struggles of an aspiring actor. In Hollywood, he learned quickly that success rarely comes easily.
Nonetheless, his persistence paid off when he landed the role of Alex P. Keaton on the popular NBC sitcom Family Ties, which debuted in 1982.
On Family Ties, Fox played the intelligent, fast‑talking, conservative‑leaning teenage son of liberal parents. His performance was both comedic and charismatic, earning him widespread praise and several awards, including multiple Emmy Awards and Golden Globes during the show’s run. The role also made him a star — not just in America, but internationally.
Breakthrough: Back to the Future and Film Success
While Fox’s television success with Family Ties firmly established him in the entertainment world, it was the 1985 blockbuster Back to the Future that turned him into a global movie star.
In the film, he portrayed Marty McFly, a teenager accidentally sent back in time in a DeLorean time machine. The role became iconic, capturing the imagination of audiences and launching a major franchise.
Fox’s work in Back to the Future required high energy, physicality, and a natural comedic timing — all of which he delivered with ease. He juggled filming for the movie with his television commitments, a feat that spoke to both his passion and work ethic.
Over the next several years, he starred in a string of successful films, including Teen Wolf, The Secret of My Success, Casualties of War, and the Back to the Future sequels.
By the age of 29, Fox had spent most of his adult life in front of the camera, winning over viewers with his mix of humor, vulnerability, and relatable charm.
A Devastating Diagnosis
In 1991, during filming on the set of Doc Hollywood, Fox began noticing a tremor in his pinky finger. What seemed at first like a minor concern was diagnosed by a neurologist as early‑onset Parkinson’s disease, a progressive neurological condition that affects movement and coordination.
He was just 29 years old — an age when most people are still building careers and planning for the future.
Parkinson’s disease is a degenerative disorder without a cure, and its symptoms — including tremors, stiffness, and difficulty with balance and speech — can worsen over time.
For someone whose life and career depended on precise movement, engaging performance, and public presence, this diagnosis was nothing short of life‑altering.
Initially, Fox kept the diagnosis private. He continued acting, including starring as Deputy Mayor Mike Flaherty on the ABC sitcom Spin City beginning in 1996, where he received further critical acclaim and awards.
Behind the scenes, however, he struggled with the reality of the disease, entering what he later would describe as several years of denial and internal conflict about his future.
Going Public and Becoming an Advocate
For years, Fox tried to manage his symptoms and maintain his career without revealing the truth about his health. Eventually, however, he realized that keeping the diagnosis secret was no longer tenable.
In 1998, during his run on Spin City, he publicly disclosed that he had Parkinson’s disease in an interview with People magazine and ABC’s Barbara Walters. This courageous decision helped break down stigma and opened up a national conversation about the disease.
The response he received — both from fans and from the broader entertainment community — was deeply supportive, emboldening Fox to shift his focus from hiding his symptoms to advocating for research and understanding. Rather than retreating from the world, he chose to use his platform to make a difference.
Two years after publicly revealing his diagnosis, in 2000, Fox founded The Michael J. Fox Foundation for Parkinson’s Research.
Today, the organization is one of the world’s leading non‑profit funders of Parkinson’s research, having raised billions of dollars and supported groundbreaking clinical studies, early‑stage therapeutic development, and the largest datasets of biosamples ever assembled for Parkinson’s research.
Fox’s foundation has also contributed to research that aims to detect the disease earlier and understand its progression more deeply — milestones that could one day lead to more effective treatments or prevention.
While a cure has not yet been found, the progress made in research has been substantial and remains a testament to sustained advocacy and investment.
Beyond Parkinson’s: Continued Career and Personal Life
Even as his symptoms gradually became more noticeable, Fox continued working in film and television. In addition to Spin City, he voiced lead characters in animated films such as Stuart Little and appeared in roles on series like Rescue Me, The Good Wife, Curb Your Enthusiasm, and The Good Fight.
His final major television project as a regular cast member was The Michael J. Fox Show from 2013 to 2014.
Over time, however, Parkinson’s symptoms made the physical demands of acting increasingly difficult. In 2020, he announced his retirement from full‑time acting due to the progression of his condition.
Though retired, Fox made a notable return to the screen, portraying a character with Parkinson’s disease in the Apple TV+ series Shrinking, demonstrating both empathy and courage in bringing an honest portrayal to audiences.
Fox’s personal life has been a grounding force through his journey. He married actress Tracy Pollan, his co‑star from Family Ties, in 1988, and they have four children together.
Fox has frequently spoken about the critical role his family has played in supporting him through the highs and lows of his health challenges and advocacy work.
Writing and Reflecting: Memoirs and Legacy
Michael J. Fox has authored several books that offer insight into his life, career, and evolving relationship with Parkinson’s disease. His first memoir, Lucky Man, chronicles his rise to fame and early years living with Parkinson’s.
The book combines candid reflections on vulnerability with his characteristic humor and philosophical insight, presenting both the high points of his success and the challenges of confronting a chronic illness.
He later published other works, including Always Looking Up and No Time Like the Future: An Optimist Considers Mortality, which explore deeper themes of resilience, mortality, and the meaning of purpose amidst adversity. These writings have resonated with readers worldwide, offering both perspective and inspiration.
In 2025, he announced a new memoir titled Future Boy, aiming to look back at his early career and the experiences that shaped him, including the joys and challenges of simultaneously filming Family Ties and Back to the Future.
Recognition and Honors
Over the course of his career and advocacy, Fox has been recognized with numerous awards. As an actor, he won multiple Emmys, Golden Globes, Screen Actors Guild Awards, and even a Grammy for contributions to entertainment.
He was inducted into the Hollywood Walk of Fame and Canada’s Walk of Fame, and he was appointed an Officer of the Order of Canada for his contributions to film and television as well as his humanitarian work.
Perhaps most notably, in 2022, Fox received the Jean Hersholt Humanitarian Award from the Academy of Motion Picture Arts and Sciences — an honorary Oscar recognizing his advocacy and philanthropic contributions in the fight against Parkinson’s disease.
The Ongoing Journey: Challenges and Perspective
Living with Parkinson’s for more than three decades has not been easy. The disease is degenerative, affecting movement, balance, coordination, and even speech.
Fox has spoken openly about the daily challenges it presents — including the emotional and physical toll — yet he approaches it with unflinching honesty and a sense of optimism that has defined his public persona.
In recent interviews, Fox has discussed how he navigates daily life with Parkinson’s, including using a wheelchair and managing his symptoms with medication and therapy.
Despite these hurdles, he continues to find meaning in family, advocacy, and creative expression. His partnership with his wife, Tracy Pollan, and their children remains a central source of strength.
A Legacy of Hope and Inspiration
Michael J. Fox’s life story is a powerful reminder that talent and success are only part of a person’s narrative. His trajectory from teenage TV star to Hollywood legend and then to a tireless advocate for Parkinson’s research reflects not only his gifts as a performer but his deep humanity, resilience, and capacity for hope.
He has shown the world that adversity — even one as challenging as a chronic, progressive disease — can be met with courage, purpose, and an unshakeable commitment to making life better for others.
In doing so, Fox has inspired millions of people living with Parkinson’s and beyond, proving that while a diagnosis might change a life, it does not have to define it.

The rain had just ended when the Good Samaritan slowed their pace along a quiet roadside in the Philippines. The sky was still heavy with gray clouds, and droplets clung to the blades of grass like tiny mirrors. The road was mostly empty, the kind of place where thoughts grow louder than footsteps. As they walked, a sound cut through the calm — a faint, uneven cry, so soft it almost blended with the wind. The Samaritan stopped, heart thudding, and listened again. The sound came once more, fragile and desperate, rising from the grassy ditch beside the road. 🌧️
They stepped closer and pushed aside the wet grass. There, half-hidden and unnaturally still, lay a yellow plastic bag. It was tied tightly at the top, its sides slightly moving. The Samaritan felt a chill that had nothing to do with the rain. They didn’t open the bag. Something deep inside warned them not to waste even a second. With shaking hands, they pulled out their phone and called BACH Project PH, a rescue group they had followed online for years, always hoping they’d never need to dial the number. 📱
The voice on the other end didn’t hesitate. Within minutes, the rescue team was on their way. When the vehicle arrived, its tires splashing through puddles, the rescuers jumped out with practiced urgency.

The bag was carefully untied, and the cries inside grew clearer — tiny, broken sounds fighting for air. Inside were five newborn kittens, eyes sealed shut, bodies tangled together, their fur damp and dirty. One rescuer sucked in a sharp breath. Another whispered, “We’ve got you now.” 🐾
The kittens were rushed to the rescue center, wrapped in towels and placed near warming pads. They were cold to the touch, dangerously so, and their tiny mouths opened and closed weakly. The team moved fast — mixing formula, checking hydration, rubbing small bodies to stimulate breathing. “They’re extremely fragile,” one rescuer said quietly. “We might’ve been minutes too late.” Bottles were offered, and slowly, miraculously, the kittens began to respond. 🍼
The first night was tense. One kitten struggled to breathe evenly, another refused to feed. Volunteers took turns watching over them, sleeping in chairs, waking every hour to feed and check temperatures. No one complained. By dawn, exhaustion hung in the air — but so did hope. All five kittens were still alive. Their cries were a little louder now, their movements slightly stronger. 🌱

That hope was tested quickly. In the same 24-hour period, nine more kittens arrived at BACH Project PH from different rescue calls. Boxes, baskets, and carriers filled every available space. Suddenly, there were fourteen tiny lives needing warmth, milk, and constant care. The team was overwhelmed, but no one suggested turning any away. “We’ll make it work,” someone said, and everyone nodded. 😿
Two foster homes stepped in, opening their doors without hesitation. Spare rooms became nurseries filled with soft blankets, heating pads, and the steady hum of quiet determination. The five kittens from the yellow bag stayed together, as if bonded by the memory of what they’d survived. They grew slowly but steadily. Eyes opened to reveal cloudy blue gazes. Tiny paws learned to push, then wobble, then run. 💛
Each kitten developed a personality. One was fearless, always the first to explore. One was gentle and quiet, happiest curled against a warm chest. Another demanded food loudly, announcing hunger to the entire house. Watching them grow felt like watching a miracle unfold day by day. The rescuers shared updates online, and messages of support poured in from around the world. 🐱

Weeks turned into months, and adoption applications began to arrive. Letting them go was harder than anyone expected. One by one, the kittens left for loving homes. The last of the five was adopted by an older woman who lived near the road where the yellow bag had been found. She named the kitten Lila and promised to keep her safe always. 🌸
Life moved on. New rescues came, new challenges followed. But the memory of the yellow bag never fully faded. Then, nearly a year later, on another rainy afternoon, the Good Samaritan found themselves walking that same road again.

The grass was taller now, the ditch deeper. As they passed the familiar spot, something caught their eye — a small shelter made from wood and tarp. Beneath it sat a healthy adult cat, her fur clean, her eyes bright. Beside her were three newborn kittens, warm and protected. 😺
The cat looked up and met the Samaritan’s gaze. Around her neck was a worn collar. Recognition struck like lightning. Lila. The woman from the nearby house soon appeared, smiling softly. “She comes here whenever she’s expecting,” she said. “I think she remembers what this place took from her — and what it gave back.” The Samaritan felt tears sting their eyes. What had begun as cruelty had ended in protection, in life guarded instead of discarded. ✨
They stepped closer and pushed aside the wet grass. There, half-hidden and unnaturally still, lay a yellow plastic bag. It was tied tightly at the top, its sides slightly moving. The Samaritan felt a chill that had nothing to do with the rain. They didn’t open the bag. Something deep inside warned them not to waste even a second. With shaking hands, they pulled out their phone and called BACH Project PH, a rescue group they had followed online for years, always hoping they’d never need to dial the number. 📱
The voice on the other end didn’t hesitate. Within minutes, the rescue team was on their way. When the vehicle arrived, its tires splashing through puddles, the rescuers jumped out with practiced urgency.
The bag was carefully untied, and the cries inside grew clearer — tiny, broken sounds fighting for air. Inside were five newborn kittens, eyes sealed shut, bodies tangled together, their fur damp and dirty. One rescuer sucked in a sharp breath. Another whispered, “We’ve got you now.” 🐾
The kittens were rushed to the rescue center, wrapped in towels and placed near warming pads. They were cold to the touch, dangerously so, and their tiny mouths opened and closed weakly. The team moved fast — mixing formula, checking hydration, rubbing small bodies to stimulate breathing. “They’re extremely fragile,” one rescuer said quietly. “We might’ve been minutes too late.” Bottles were offered, and slowly, miraculously, the kittens began to respond. 🍼
The first night was tense. One kitten struggled to breathe evenly, another refused to feed. Volunteers took turns watching over them, sleeping in chairs, waking every hour to feed and check temperatures. No one complained. By dawn, exhaustion hung in the air — but so did hope. All five kittens were still alive. Their cries were a little louder now, their movements slightly stronger. 🌱
That hope was tested quickly. In the same 24-hour period, nine more kittens arrived at BACH Project PH from different rescue calls. Boxes, baskets, and carriers filled every available space. Suddenly, there were fourteen tiny lives needing warmth, milk, and constant care. The team was overwhelmed, but no one suggested turning any away. “We’ll make it work,” someone said, and everyone nodded. 😿
Two foster homes stepped in, opening their doors without hesitation. Spare rooms became nurseries filled with soft blankets, heating pads, and the steady hum of quiet determination. The five kittens from the yellow bag stayed together, as if bonded by the memory of what they’d survived. They grew slowly but steadily. Eyes opened to reveal cloudy blue gazes. Tiny paws learned to push, then wobble, then run. 💛
Each kitten developed a personality. One was fearless, always the first to explore. One was gentle and quiet, happiest curled against a warm chest. Another demanded food loudly, announcing hunger to the entire house. Watching them grow felt like watching a miracle unfold day by day. The rescuers shared updates online, and messages of support poured in from around the world. 🐱
Weeks turned into months, and adoption applications began to arrive. Letting them go was harder than anyone expected. One by one, the kittens left for loving homes. The last of the five was adopted by an older woman who lived near the road where the yellow bag had been found. She named the kitten Lila and promised to keep her safe always. 🌸
Life moved on. New rescues came, new challenges followed. But the memory of the yellow bag never fully faded. Then, nearly a year later, on another rainy afternoon, the Good Samaritan found themselves walking that same road again.
The grass was taller now, the ditch deeper. As they passed the familiar spot, something caught their eye — a small shelter made from wood and tarp. Beneath it sat a healthy adult cat, her fur clean, her eyes bright. Beside her were three newborn kittens, warm and protected. 😺
The cat looked up and met the Samaritan’s gaze. Around her neck was a worn collar. Recognition struck like lightning. Lila. The woman from the nearby house soon appeared, smiling softly. “She comes here whenever she’s expecting,” she said. “I think she remembers what this place took from her — and what it gave back.” The Samaritan felt tears sting their eyes. What had begun as cruelty had ended in protection, in life guarded instead of discarded. ✨


A social worker with twenty years of experience dealing with cases just like mine. Gloria had seen it all—the broken families, the lies spun by siblings, the parents who’d rather believe a convenient story than face uncomfortable truths. She knew the signs and symptoms of hypothermia, but more importantly, she recognized the signs of familial betrayal.
Gloria found me sprawled on the gravel, a sodden, shivering mess. Her instincts kicked in immediately. She had a woolen blanket in her car—something she always carried for emergencies—and she wrapped it around me with practiced care. As she waited for the ambulance, she talked to me even though I was unconscious, hoping that perhaps on some level, I could hear her calming words.
When the paramedics arrived, Gloria was already on the phone with the police, recounting what she had found. The officer on the line had listened intently, his tone growing more serious with each detail she provided. This wasn’t just a case of a lost girl in a storm—it was shaping up to be something much darker.
At the hospital, they brought me back from the brink. I remember waking up to the steady beep of machines, the sterile smell of antiseptic, and the warmth of heated blankets cocooning me. My body felt heavy, weighted by exhaustion and the remnants of cold. But most of all, I felt an overwhelming sense of safety—a sensation I hadn’t realized I was missing until it returned.
When my father arrived, he was met not just by the hospital staff, but by Officer Daniels and Gloria. They stood as a united front, their eyes fixed on him with a mixture of judgment and expectation. My father, who always had an answer for everything, seemed at a loss. The lies he’d accepted from Karen were falling apart under scrutiny, and for the first time, he was being held accountable.
Karen stayed silent, shadows of fear flickering across her face. She was so used to being the favored child, the one whose word was gold. But now, the truth was creeping in, threatening to unravel everything she had constructed.
Gloria turned to me, her eyes softening. “You’re safe now,” she said gently, as if willing me to believe it. In her presence, I felt a flicker of hope. It was fragile, easily quashed, but there nonetheless.
The aftermath was a whirlwind. Social services, investigations, truths laid bare. The world I knew shifted and reshaped itself. Gloria, true to her profession, advocated for me tirelessly. She ensured I wouldn’t return to a house where lies were accepted over love.
In the weeks that followed, I stayed with Gloria temporarily. Her home was warm and filled with laughter—something I realized I had sorely missed. She was more than a rescuer; she became a mentor, a guide in navigating the complexities of a life I thought was unchangeable.
My father’s words, meant to wound, had instead propelled me into a new reality. And though the path wasn’t easy, it was mine to walk, with Gloria by my side, teaching me to trust again.
I often wonder if my sister ever understood the depth of her actions. If my father ever regretted his words. But as I sat in Gloria’s home, the storm outside nothing but a memory, I learned to let go. I was rebuilding, one day at a time, stronger and more resilient than before.


As the realization settled in, a painful knot formed in my stomach. The very thought of my son or daughter-in-law being responsible for this was unbearable. But there was no denying the evidence. The bruises on Liam’s fragile body screamed of a darkness that had to be brought to light.
I spent that sleepless night in the hospital, my mind racing with a mix of dread and resolve. I loved Jared and Amanda, but Liam’s safety had to be my priority. It was a battle between the love for my child and the desperate need to protect my grandson. It was a battle I never imagined I would have to fight.
The authorities were involved by morning. A detective and a child protective services worker sat across from me in a small, sterile conference room. Their questions were pointed, and I knew the weight of my answers could change everything for our family.
“Has Jared or Amanda ever shown signs of aggression?” the detective asked gently.
I hesitated, memories flooding back. Jared had always been a gentle soul, but in recent months, I’d noticed a strain in his voice, a tension in his shoulders. Amanda seemed overwhelmed, often speaking in clipped tones. But did that mean they were capable of hurting Liam?
“No,” I finally replied, my voice barely above a whisper. “But… the bruises. They can’t be ignored.”
Liam was kept in the hospital for observation while the investigation began. I visited him as often as I could, each time overwhelmed by the innocence in his eyes. He was so small, so vulnerable, and yet so incredibly strong.
As the days stretched into a week, I prepared myself for the fallout. Jared and Amanda were interviewed separately. Their explanations were vague, filled with confusion and denial. They claimed the bruises must have happened at daycare, or perhaps during a moment of clumsiness, but their words lacked conviction.
One afternoon, as I sat by Liam’s hospital crib, Jared walked in. He looked older, more haggard, than I’d ever seen him. He stood by the door, tears brimming in his eyes.
“Mom,” he said, his voice cracking. “We would never hurt him. You have to believe me.”
I wanted to comfort him, tell him everything would be alright, but the image of Liam’s bruises haunted me. I took a deep breath, choosing my words carefully.
“I want to believe you, Jared. I really do. But until we find out what’s happening, we have to keep Liam safe.”
The tears spilled over then, and he nodded, wiping his eyes with the back of his hand. “I just want him to be okay.”
It was the most honest thing he could have said, and for the first time, I saw a glimmer of hope. Maybe this was the wake-up call they needed. Maybe, just maybe, they could find a way to heal — as individuals, as parents, and as a family.
In the meantime, I would be there for Liam, doing everything in my power to ensure his safety. Even if it meant confronting the unthinkable, even if it meant standing against my own son, I would not back down. Because sometimes, love means making the hardest choices. And for Liam, I would choose him every time.


It was Ethan, my grandson. His grip was firm, but his eyes were softer than I’d ever seen them. They shimmered with something I couldn’t immediately identify—was it regret, sadness, love? Maybe all three. He held my gaze firmly, and the laughter in the room ceased to exist for me. His voice was barely above a whisper but carried the weight of conviction. “Wait, Grandma.”
His voice rose, now addressing the entire room. “You don’t understand. This isn’t just a quilt.” His voice was steady, filled with an emotion that silenced the echoes of mocking laughter. “This is a tapestry of my history, our family’s history.” He turned to Veronica, his bride, and his voice softened. “When you laugh at it, you’re laughing at everything that made me who I am.”
The room was silent, save for the faint clinking of glasses and shifting of uncomfortable bodies. Veronica’s face flushed, perhaps from embarrassment or realization, and she looked down, visibly humbled. Ethan continued, his voice gathering strength. “This quilt is a gift far more valuable than anything money could buy. It’s a piece of Grandma Maggie’s life, and now it’s a piece of ours. Each stitch is a story, a memory.” He touched the fabric reverently, pointing out each distinct patch. “This is from my baby blanket, this from my first school uniform… and this,” he said, tracing the lace with his finger, “is from Grandma’s wedding veil.”
As he spoke, the atmosphere in the room shifted, electricity charging the air. Whispers circulated among the guests, but now they were filled with admiration and reflection, not derision. Slowly, the hum of voices was replaced by the sound of polite applause, then a standing ovation. The orchestra, sensing the change in mood, began to play softly, a melody as gentle and heartfelt as my grandson’s words.
Veronica, eyes tearful, reached for the microphone. “I’m so sorry, Grandma Maggie,” she said, her voice trembling with sincerity. “I didn’t understand. This is the most beautiful gift. Thank you.”
My heart, moments ago heavy with humiliation, now surged with pride and warmth. Ethan enveloped me in a hug, whispering, “You’ve always been my greatest role model, Grandma.”
The rest of the evening unfolded like a dream. Guests approached me with stories of their own cherished family heirlooms, of the value of love and memory over material wealth. I was hugged, apologized to, and celebrated in a way I had never anticipated. The quilt became a centerpiece, a conversation starter, and a reminder of what truly matters.
As the evening wound down and I prepared to return to my quiet life, Ethan and Veronica approached me once more. They promised to visit soon, to learn from the stories captured within the quilt and to create more memories to add to it.
Life, it seemed, still had lessons to teach me—lessons about love, resilience, and the power of an open heart. And as I left the opulent hall, I realized that this day, which began with laughter at my expense, ended with something far richer: a reminder of the enduring strength of family and the quiet, yet profound, impact of love.

At some point in your life, you might experience a very flustering sexual encounter: You’re about to get down and dirty with your partner, when all of a sudden they lose their erection, or they can’t get one up in the first place. It leaves you unsure of what to do next — do you just keep going because you bought new lacy underwear for this, or do you cancel the evening’s sexcapades entirely? Plus, there’s probably a small voice in your head telling you that you did something wrong, or that this change in mood is your fault. (Let’s clear that up now: it’s obviously not!)
Difficulty keeping an erection sufficient for penetration is referred to as Erectile Dysfunction, or ED for short. Here’s the thing: this is a pretty normal issue, whether it happens just once or numerous times in a row. People of all sexes experience difficulty with arousal, and it’s inevitable that this comes up during intimacy. Issues with arousal are unrelated to how explosively sexy your relationship is or how much you love each other — sometimes there’s just no lift off for a variety of reasons.
That said, you’re not doomed to figure this out on your own. To help your partner address their ED, it’s crucial to discover the cause of it — so get ready to communicate. Here’s what might be preventing them from getting hard and how to address it.
There are sometimes physical causes at play.
There is a whole host of physical health issues that can lead to ED, explains Dr. Alex Chinks, Boston-based licensed clinical psychologist and sexologist. These could include:
Diabetes
High blood pressure
Obesity
Fatigue
Smoking
High cholesterol
Advanced age
ED can even be an early symptom of current or future heart disease, Dr. Chinks says.
The first thing Dr. Chinks asks her ED patients: “When was your last physical?” — in order to rule out these medical causes. “My next question is about alcohol and drug use,” Dr. Chinks continues. “Drinking is the largest culprit of ED in men under the age of 40. And any recreational or prescription drugs can bring about ED as a side effect.”
Maybe it’s all mental.
ED gets a lot more complicated when it comes to psychological causes, because humans are emotional, sensitive, insecure creatures (yes, all of us!). Your significant other might have an image in their mind of how sex should look and how they should perform — but when real life doesn’t meet their expectations, this can lead to stress and going limp as a physical reaction. Your partner might also lose an erection due to reasons ranging from anxiety to big life changes. Depression in general can dampen sex drive and increase the chance that erection loss keeps occurring. (Frustratingly, antidepressants can lower libido and lead to ED as well.)
“I often say that one’s sex life is a window into their non-sexual lives,” Dr. Chinks says. That means if there’s a lot going on internally, ED and other sexual issues can come as a result.
Or there’s a sexual dysfunction present.
“Our sexual response cycle typically follows a pathway of desire-arousal-excitement-orgasm,” Dr. Chinks says, where erections are a sign of arousal. “If your partner is experiencing low desire (or libido)” — the first step in the process — “then they may not be able to move into the arousal zone.” Sometimes you’re just not feeling that horny, and that’s OK. But on the chance that there is sexual dysfunction at play, a doctor’s visit never hurts to figure out what’s up.
6 ways to deal with ED in a relationship
You can still have a satisfying sex life when a partner is experiencing ED — we promise. Here are a few strategies to get you there:
Get creative. Keep in mind that erections are not going to make or break your sex life. And for most people with a clit, penetration is not even needed for pleasure. Especially if you care a lot about your partner, there are other ways to satisfy, and sex consist of a whole range of behaviors. Try mutual masturbation or playing with toys while centering other erogenous zones, like the clitoris, anus, or prostate.
Play with it soft. Marriage and family therapist Brooke Norton says that playing with a soft penis can be enjoyable for everyone. “A soft penis is just that — it doesn’t mean anything about masculinity or being a good lover,” she tells SheKnows. “And we also have hands, mouths, and the rest of our bodies to use for pleasure.” The possibilities are endless, whether there’s an erection present or not.
Take a break. Dr. Emily Morse, Doctor of Human Sexuality and host of the popular Sex With Emily podcast, recommends a tactic in the same vein. “Try taking a break from [penetrative] sex for a bit – go back to kissing, have him go down on you and touch each other’s bodies, have a snack — whatever it is, the mood can come back!”
Redefine what sex means to you. If you and your partner are still feeling totally lost about what to do next, there are a few things to try when working past ED. “I often encourage folks to think about what sex is about,” Norton says. “Is it really about staying hard? Sex is about sharing pleasure and enjoyment, not necessarily about parts behaving in a particular way. Some of us were taught that there is foreplay and then penetration is the main event.” Instead, think of every part of a sexual encounter as sex. There’s no need to stick to a script when there are so many broad ways to express yourself sexually.
Talk to an expert. Oftentimes, a sex therapist will also be able to come up with suggestions and assist with matters of ED. It’s important for a professional to give attention to individual stories and unique circumstances that brought people to the point where things are a problem. Norton says, “I once worked with a cis, hetero couple who really prioritized her penetration, so I asked them to consider using a toy for this purpose. It turned out that he enjoyed using the toy on her so much that he was able to get an erection.”
Be patient and communicate. Overall, the best way you can help your partner is to be understanding and patient, and to not get upset in any way (remember, this isn’t your fault — or theirs). In our very patriarchal culture, it can feel like a partner’s erection is inherently related to your appearance, sexual prowess, and desirability, but that’s not true. Keep in mind that ED can feel embarrassing and your partner can feel like they’re taking a hit to their self-esteem as well, so just try to be the most supportive person you can. Being able to talk about and work through this will set you up for an even stronger relationship.
Difficulty keeping an erection sufficient for penetration is referred to as Erectile Dysfunction, or ED for short. Here’s the thing: this is a pretty normal issue, whether it happens just once or numerous times in a row. People of all sexes experience difficulty with arousal, and it’s inevitable that this comes up during intimacy. Issues with arousal are unrelated to how explosively sexy your relationship is or how much you love each other — sometimes there’s just no lift off for a variety of reasons.
That said, you’re not doomed to figure this out on your own. To help your partner address their ED, it’s crucial to discover the cause of it — so get ready to communicate. Here’s what might be preventing them from getting hard and how to address it.
There are sometimes physical causes at play.
There is a whole host of physical health issues that can lead to ED, explains Dr. Alex Chinks, Boston-based licensed clinical psychologist and sexologist. These could include:
Diabetes
High blood pressure
Obesity
Fatigue
Smoking
High cholesterol
Advanced age
ED can even be an early symptom of current or future heart disease, Dr. Chinks says.
The first thing Dr. Chinks asks her ED patients: “When was your last physical?” — in order to rule out these medical causes. “My next question is about alcohol and drug use,” Dr. Chinks continues. “Drinking is the largest culprit of ED in men under the age of 40. And any recreational or prescription drugs can bring about ED as a side effect.”
Maybe it’s all mental.
ED gets a lot more complicated when it comes to psychological causes, because humans are emotional, sensitive, insecure creatures (yes, all of us!). Your significant other might have an image in their mind of how sex should look and how they should perform — but when real life doesn’t meet their expectations, this can lead to stress and going limp as a physical reaction. Your partner might also lose an erection due to reasons ranging from anxiety to big life changes. Depression in general can dampen sex drive and increase the chance that erection loss keeps occurring. (Frustratingly, antidepressants can lower libido and lead to ED as well.)
“I often say that one’s sex life is a window into their non-sexual lives,” Dr. Chinks says. That means if there’s a lot going on internally, ED and other sexual issues can come as a result.
Or there’s a sexual dysfunction present.
“Our sexual response cycle typically follows a pathway of desire-arousal-excitement-orgasm,” Dr. Chinks says, where erections are a sign of arousal. “If your partner is experiencing low desire (or libido)” — the first step in the process — “then they may not be able to move into the arousal zone.” Sometimes you’re just not feeling that horny, and that’s OK. But on the chance that there is sexual dysfunction at play, a doctor’s visit never hurts to figure out what’s up.
6 ways to deal with ED in a relationship
You can still have a satisfying sex life when a partner is experiencing ED — we promise. Here are a few strategies to get you there:
Get creative. Keep in mind that erections are not going to make or break your sex life. And for most people with a clit, penetration is not even needed for pleasure. Especially if you care a lot about your partner, there are other ways to satisfy, and sex consist of a whole range of behaviors. Try mutual masturbation or playing with toys while centering other erogenous zones, like the clitoris, anus, or prostate.
Play with it soft. Marriage and family therapist Brooke Norton says that playing with a soft penis can be enjoyable for everyone. “A soft penis is just that — it doesn’t mean anything about masculinity or being a good lover,” she tells SheKnows. “And we also have hands, mouths, and the rest of our bodies to use for pleasure.” The possibilities are endless, whether there’s an erection present or not.
Take a break. Dr. Emily Morse, Doctor of Human Sexuality and host of the popular Sex With Emily podcast, recommends a tactic in the same vein. “Try taking a break from [penetrative] sex for a bit – go back to kissing, have him go down on you and touch each other’s bodies, have a snack — whatever it is, the mood can come back!”
Redefine what sex means to you. If you and your partner are still feeling totally lost about what to do next, there are a few things to try when working past ED. “I often encourage folks to think about what sex is about,” Norton says. “Is it really about staying hard? Sex is about sharing pleasure and enjoyment, not necessarily about parts behaving in a particular way. Some of us were taught that there is foreplay and then penetration is the main event.” Instead, think of every part of a sexual encounter as sex. There’s no need to stick to a script when there are so many broad ways to express yourself sexually.
Talk to an expert. Oftentimes, a sex therapist will also be able to come up with suggestions and assist with matters of ED. It’s important for a professional to give attention to individual stories and unique circumstances that brought people to the point where things are a problem. Norton says, “I once worked with a cis, hetero couple who really prioritized her penetration, so I asked them to consider using a toy for this purpose. It turned out that he enjoyed using the toy on her so much that he was able to get an erection.”
Be patient and communicate. Overall, the best way you can help your partner is to be understanding and patient, and to not get upset in any way (remember, this isn’t your fault — or theirs). In our very patriarchal culture, it can feel like a partner’s erection is inherently related to your appearance, sexual prowess, and desirability, but that’s not true. Keep in mind that ED can feel embarrassing and your partner can feel like they’re taking a hit to their self-esteem as well, so just try to be the most supportive person you can. Being able to talk about and work through this will set you up for an even stronger relationship.


The atmosphere in the Grand Ballroom shifted from one of eager anticipation to stunned silence. Guests exchanged bewildered glances, their attention riveted on the bride who had so unexpectedly seized the microphone. My heart pounded in my chest, but my resolve was unwavering. This was not the moment anyone expected, but it was the moment I needed.
“Marriage is built on love and trust,” I continued, my voice steady and clear. “But sometimes, it unveils truths we cannot ignore.” I felt the weight of every pair of eyes in the room upon me, but I focused on Mrs. Patricia, whose painted smile faltered under the scrutiny of the crowd. Chloe’s face paled beside her mother, and Brandon’s confident facade started to crack.
With a calmness that belied the storm within, I played the recording. Patricia’s venomous words filled the air, each syllable a betrayal louder than the last. Gasps and murmurs rippled through the guests as they absorbed the reality of the situation. The façade of a perfect family shattered like glass, the shards reflecting a truth far uglier than the pristine, golden setting of the ballroom.
Brandon’s face turned a shade of crimson, his eyes darting from me to his mother, who sat frozen, her expression now one of genuine disbelief. For an eternal moment, the world held its breath, the grandeur of the setting at odds with the depths of deceit unveiled.
As the final words of Patricia’s plan echoed and faded into silence, I lowered the microphone and faced Brandon. His lips parted as if to perform a well-rehearsed denial, but I raised a hand to stop him.
“I loved you, Brandon. I thought we were building a life together,” I said, the edge of vulnerability now unmistakable in my voice. “But I see now that I was merely a pawn in your family’s game. There will be no merger, no marriage, and rest assured, no trust fund for you.”
The room held its collective breath, watching the saga unfold like a drama on stage. My father’s presence, a towering figure of authority and power, gave me strength. I could feel his unwavering support as a silent promise that I would not face this alone.
Turning to the guests, I offered a small, sincere smile. “Thank you all for being here today. I apologize for the unexpected turn of events, but as I’ve learned, life is unpredictable.”
With one last, parting glance at the family that almost trapped me, I handed the microphone back to the priest, who looked as though he might faint. The doors at the end of the aisle, once a pathway to a future I’d envisioned with love, now stood as my gateway to freedom and self-discovery.
I walked back down the aisle, head held high. Each step was a reclaiming of my world, a testament to my strength and resilience. The whispers and stares no longer mattered. I was no longer the naïve bride-to-be but a woman empowered by truth and liberation.
Outside, the city awaited, full of possibilities and new beginnings. I inhaled deeply, the crisp air filling me with renewed determination. Today was not the end but the beginning of a journey I would forge on my own terms. A journey where I would love, trust, and believe in myself above all else.